Best Dental Treatments
Dr. Bhutani Dental Group provides you with the best dentist in Delhi NCR. Our clinics are equipped with top dental infrastructure, technology, and care facilities to ensure that you get the best dental treatments. Whether you’re experiencing pain or looking for dentures, we provide all types of dental treatments.







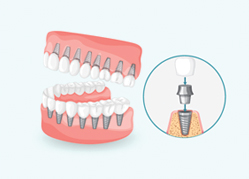



















Implant Systems
Dental implants are bio compatible metal anchors surgically positioned in the jaw bone. It acts as an artificial tooth root. As India’s best dental implant clinic, we’re driven by our vision to provide the best quality dental implant to our visitors at an affordable range. We offer efficient and globally recognized dental implant systems.










